Diabetic Retinopathy
If you or a loved one has diabetes, regular eye care becomes an even more important part of your overall health routine. Diabetic retinopathy is a common eye condition that affects individuals with Type 1 and Type 2 diabetes, developing in more than half of those living with diabetes. However, early detection and proper treatment can effectively preserve your vision.
At Retina Consultants of Southern Colorado, we specialize in comprehensive care for retinal conditions, including prevention, diagnosis, and treatment, helping patients maintain healthy vision for years to come. Learn more about this condition and how our team of providers can help protect your sight.
What Is Diabetic Retinopathy?
Diabetic retinopathy is a complication of diabetes that affects the retina, the thin, light-sensitive layer of tissue at the back of the eye responsible for sharp, detailed vision. Elevated blood sugar levels damage the small blood vessels in the retina, causing them to leak, swell, or close off completely. This condition is the most common cause of irreversible blindness among working-age adults and occurs in more than half of people with diabetes.
Stages of Diabetic Retinopathy
Diabetic retinopathy progresses through two distinct stages, each requiring different levels of monitoring and treatment.
This earlier, more common stage occurs when blood vessel walls in the retina weaken due to high blood sugar levels. Tiny bulges form on smaller vessels, which can then swell and leak fluid into the retina. Larger vessels may swell and become irregular in width. This condition can progress from mild to severe as more blood vessels become damaged.
A key complication during this stage is macular edema, or fluid buildup in the macula, the retina's center, responsible for sharp vision. When this affects sight, prompt treatment is needed to prevent permanent vision loss.
Symptoms and Warning Signs
Diabetic retinopathy often develops silently, and you may not notice you have it until significant damage has been done. This is why early detection is crucial. Here are some symptoms to look out for:
- Blurred or distorted vision
- Difficulty reading or recognizing faces
- Trouble seeing colors correctly
- The appearance of floaters (small spots that drift through your vision)
- Dark shadows or empty areas in your vision
- Sudden vision loss
If you experience any of these symptoms in one or both eyes, schedule an eye exam immediately.
Risk Factors
While anyone with diabetes can develop diabetic retinopathy, the risk increases with:
- Disease duration (the longer someone has diabetes, the greater the risk of developing diabetic retinopathy)
- Poor blood sugar control over time
- High blood pressure
- High cholesterol
- Pregnancy
Managing your diabetes and attending regular eye exams can significantly reduce your risk and preserve your vision.
How Is Diabetic Retinopathy Diagnosed?
Because many of the changes that occur with diabetic retinopathy don't cause symptoms until damage has been done, the best way to detect diabetic retinopathy is with a comprehensive dilated eye exam performed by an eye care specialist. During this exam, they will use eye drops to dilate your pupils, allowing a clear view of the inside of your eye and retinal tissue.
They will look for signs of the condition, such as swelling in the retina, evidence of poor retinal blood circulation, abnormal blood vessels, new blood vessels, or scar tissue.
Your doctor may also use additional diagnostic tools such as:
- Optical Coherence Tomography (OCT): High-resolution imaging that shows retinal thickness, swelling, or fluid buildup.
- Fundus Photography: Detailed photos of the retina to monitor the disease and track disease progression.
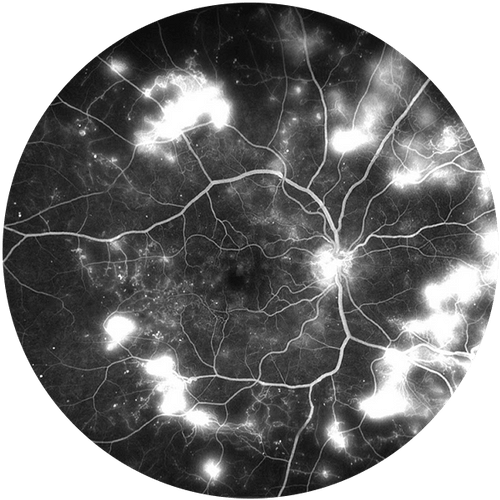
- Fluorescein Angiography (FA): A special dye is injected into your bloodstream to highlight blood vessel abnormalities in the retina, including vessels that are closed, damaged, or leaking.
These tests help identify early changes, determine severity, and guide treatment, such as how frequently follow-up examinations will be required.
Treatment Options
While diabetic retinopathy cannot be cured, effective treatments can slow progression and preserve your vision. However, some damage cannot be reversed once it becomes severe, which is why early intervention and treatment are crucial.
Treatment options depend on the stage and severity of your condition and may include:
- Intravitreal Injections: Anti-VEGF (vascular endothelial growth factor) or steroid medications are injected directly into the eye to reduce swelling, block abnormal vessel growth, and prevent vision loss. Anti-VEGF injections are often the first-line treatment for diabetic macular edema and are typically more effective than laser therapy alone.
- Laser Therapy (Panretinal Photocoagulation or PRP): Laser treatment is used to shrink abnormal blood vessels and prevent further damage in proliferative diabetic retinopathy. This is often done in combination with injections.
- Vitrectomy Surgery: In advanced cases, such as vitreous hemorrhage (bleeding into the eye's gel-like center) or retinal detachment, vitrectomy surgery may be required. This procedure removes the blood-filled vitreous gel and scar tissue to restore or preserve vision.
With timely treatment, many patients can stabilize or even improve their vision. For patients experiencing more severe vision changes, our team can also connect you with vision rehabilitation services and a variety of tools to help make everyday living with this condition more manageable.
Preventive Measures
The best defense against diabetic retinopathy is taking proactive steps to protect your vision before problems develop. By focusing on two key areas — blood sugar management and regular eye exams — you can significantly reduce your risk and catch any changes early.
Managing Blood Sugar Levels
Maintaining healthy glucose levels and keeping your hemoglobin A1C within target ranges can not only prevent the development of diabetic retinopathy but may also help existing retinopathy improve over time.
Your risk of developing diabetic retinopathy increases significantly with poorly controlled blood sugar levels and longer duration of diabetes. However, not everyone with diabetes will develop this eye condition. If you have prediabetes or other risk factors for diabetes, taking preventive action now can make a significant difference.
If you have diabetes, the National Eye Institute recommends following the TRACK approach:
- Take medications as prescribed
- Reach and maintain a healthy weight
- Add physical activity daily
- Control A1C, blood pressure, and cholesterol
- Kick the smoking habit
Scheduling Regular Eye Exams
Regular comprehensive eye exams with an eye care specialist are crucial because diabetic retinopathy often develops without noticeable symptoms in its early stages. This is especially important if you have a family history of diabetes, as having first-degree relatives (parents, siblings, or children) with diabetes significantly increases your own risk. Early detection through routine screening allows for timely intervention when treatments are most effective.
Advanced Care for Diabetic Retinopathy in Southern Colorado
If you have diabetes, don’t wait for symptoms to appear. The earlier diabetic retinopathy is caught, the better your chances of preserving your vision. At Retina Consultants of Southern Colorado, our board-certified retina specialists provide state-of-the-art diagnostic testing, individualized treatment, and compassionate care.
Call us today to schedule a comprehensive eye exam. Your sight is worth it.