Retinal Vein Occlusion: Blocked Blood Vessels in the Eye
Have you recently experienced sudden blurry vision or blind spots in your sight? While many eye conditions develop gradually, retinal vein occlusion can strike seemingly out of nowhere, leaving you concerned and confused about what's happening. Retinal vein occlusion occurs when blood vessels in your retina become blocked, similar to how a blocked artery can cause a stroke or heart attack.
The good news is that with proper diagnosis and treatment, many patients can preserve their vision and prevent further complications. At Retina Consultants of Southern Colorado, our retina specialists have extensive experience diagnosing and managing both types of retinal vein occlusion, helping patients navigate treatment options and protect their sight for the long term.
BRVO vs. CRVO: Understanding the Two Types
Retinal vein occlusion isn't a one-size-fits-all condition — it comes in two main types, and understanding the difference matters because they affect your vision differently and may require different treatment approaches.
Both types of retinal vein occlusion involve blocked veins that prevent proper blood drainage from your retina, causing blood and fluid to leak into the retinal tissue. The key difference is scope: BRVO affects a neighborhood, while CRVO affects the whole city.
Think of your retinal veins like branches on a tree. A branch retinal vein occlusion happens when one of the smaller "branch" veins gets blocked. This affects only a portion of your retina, or the section served by that particular vein. It's the more common of the two types, accounting for about 80% of all retinal vein occlusions.
Because only part of your retina is affected, you might experience vision problems in just one area of your visual field. If the blockage occurs away from your macula (the central part of your retina responsible for detailed vision), you might not notice significant symptoms at all. However, if it happens near or affects the macula, you'll likely experience more noticeable vision changes.
What Causes Retinal Vein Occlusion? Who's at Risk?
Retinal vein occlusions are usually the result of underlying health conditions affecting your blood vessels. Understanding your risk factors can help you take preventive measures and catch problems early.
Primary Risk Factors:
- High Blood Pressure (Hypertension): Chronic high blood pressure damages and hardens blood vessel walls throughout your body, including the tiny vessels in your eyes. When vessel walls thicken, blood flow can become restricted or blocked.
- Atherosclerosis and High Cholesterol: Just like plaque can build up in the arteries of your heart, it can also affect the blood vessels in your eyes. This hardening and narrowing of vessels increases the likelihood of blockages.
- Diabetes: Elevated blood sugar levels over time damage blood vessels and make them more prone to clotting and blockage. If you have diabetes, you're already at higher risk for various eye problems, and retinal vein occlusion is one of them.
- Glaucoma: Increased pressure inside the eye can compress blood vessels and contribute to blockages, particularly in CRVO cases.
- Blood Clotting Disorders: Conditions that make your blood more likely to clot — whether inherited or acquired — naturally increase your risk of vein occlusions anywhere in your body, including your eyes.
Other Risk Factors Include:
- Age over 50 (risk increases with each decade)
- Smoking
- Obesity
- Cardiovascular disease
- Inflammatory conditions
- Certain medications that affect blood clotting
- Rare causes in younger patients, such as blood disorders or vasculitis
Retinal vein occlusion may be a wake-up call about your overall vascular health. Many patients discover they have uncontrolled high blood pressure or other systemic conditions only after experiencing a vein occlusion in their eye.
Retinal Vein Occlusion Symptoms
The symptoms of retinal vein occlusion typically appear suddenly, though they may develop over the course of hours or days. What you experience depends on which type you have and how severely your retina is affected.
Common Symptoms include:
- Sudden Blurry or Distorted Vision: This is the most frequent complaint. Your vision might go from clear to fuzzy seemingly overnight. In BRVO, the blurriness may be confined to one section of your vision, while CRVO typically causes more widespread blur.
- Blind Spots or Dark Areas: You might notice a specific area in your vision where you can't see clearly or at all. This corresponds to the part of your retina affected by the blockage.
- Vision Loss: In more severe cases, particularly with CRVO, you may experience significant vision loss in the affected eye. This can range from mild to severe.
- Floaters: Some patients notice new floaters, specks, or cobwebs drifting across their vision, which can occur if bleeding happens in the eye.
The key characteristic is that these changes happen quickly. You might wake up one morning with blurry vision, or notice it suddenly while going about your day. This sudden onset is what distinguishes vein occlusion from gradually progressive conditions like cataracts or macular degeneration.
Don't ignore sudden vision changes. Even if they seem mild, prompt evaluation can make a significant difference in your outcome.
How Retinal Vein Occlusion Is Diagnosed
Diagnosing retinal vein occlusion requires a comprehensive eye exam and specialized imaging. To fully understand what's happening in your eye, your retina specialist will use several advanced diagnostic tools. Here are a few:
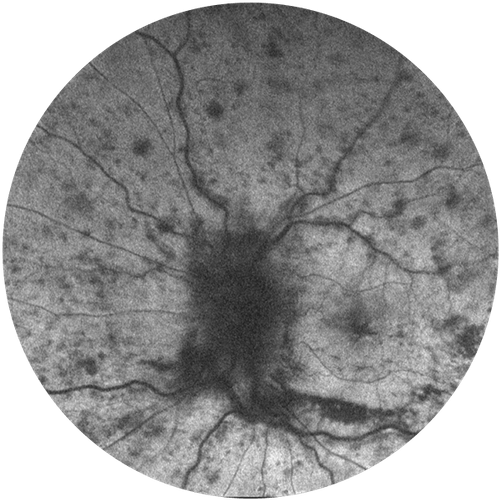
- Dilated Eye Exam: First, your doctor will dilate your pupils with eye drops to get a clear view of your retina. Using specialized lenses and lights, they can often see the telltale signs of a vein occlusion, like areas of retinal hemorrhaging (bleeding), swelling, and abnormal blood vessels.
- Optical Coherence Tomography (OCT): This high-resolution imaging technique creates detailed cross-sectional pictures of your retina, allowing your doctor to see exactly how much swelling is present, particularly in your macula. This is crucial for determining treatment and monitoring your response over time.
- Fluorescein Angiography (FA): For this test, a special dye is injected into a vein in your arm. As the dye travels through your bloodstream and into the blood vessels of your eye, your doctor takes a series of photographs. This highlights areas of leakage, poor circulation, and abnormal blood vessel growth. It's particularly helpful for identifying areas that may need laser treatment.
- OCT Angiography (OCTA): This newer technology provides detailed images of blood flow in your retina without requiring an injection. It's useful for detecting areas of poor circulation and abnormal vessel growth.
Your doctor will also want to assess your overall health, as retinal vein occlusion often signals underlying medical conditions. Expect questions about your blood pressure, cholesterol, diabetes control, and cardiovascular health. You may be referred to your primary care physician or a specialist to help manage these conditions, as controlling them is a critical part of preventing future occlusions.
Retinal Vein Occlusion Treatment Options
While we can't physically "unblock" a retinal vein that's already occluded, we can effectively treat the complications that arise from the blockage, like swelling and abnormal blood vessel growth. Treatment is personalized based on the type and severity of your vein occlusion.
This is the most common and effective treatment for the vision-threatening swelling (macular edema) that often accompanies retinal vein occlusion. When blood vessels are blocked, your eye produces a protein called VEGF (vascular endothelial growth factor) in response to the lack of oxygen. This protein causes fluid to leak from blood vessels and can trigger the growth of abnormal new vessels.
Anti-VEGF medications are injected directly into your eye to block this protein. This reduces swelling in the macula and prevents abnormal vessel growth. The injections are given in the office after your eye is numbed with anesthetic drops, and while the idea sounds intimidating, most patients report only mild discomfort.
Treatment typically starts with monthly injections for the first few months, then may be spaced out based on how your eye responds. Some patients need ongoing injections for months or even years, while others stabilize and require less frequent treatment.
Long-Term Outlook and the Importance of Ongoing Care
Retinal vein occlusion is a chronic condition that requires long-term management and monitoring. Your visual outcome depends on several factors.
For BRVO: Many patients with branch vein occlusions respond well to treatment and can maintain or even improve their vision, particularly if the macula wasn't severely affected initially. Some patients recover most of their vision, while others experience permanent changes. The key is consistent treatment and follow-up.
For CRVO: Central vein occlusions tend to be more challenging. Outcomes vary widely depending on the severity of the blockage and how well blood flow is maintained. Some people recover significant vision with treatment, while others experience lasting vision loss despite our best efforts. That said, even in cases where vision doesn't fully recover, treatment often prevents further deterioration and serious complications.
Advanced Care for Retinal Vein Occlusion in Southern Colorado
Retinal vein occlusion is a serious condition, but it's far from hopeless. With prompt diagnosis, appropriate treatment, and diligent follow-up care, many patients maintain functional vision and prevent serious complications. The most important things you can do are recognize symptoms early, seek immediate care when vision changes occur, commit to your treatment plan, and take control of your overall vascular health.
At Retina Consultants of Southern Colorado, we understand that managing retinal vein occlusion can feel overwhelming. Our experienced team is here to guide you through every step — from diagnosis and treatment to long-term monitoring and support. We use the latest diagnostic technology and evidence-based treatments to give you the best possible outcome. If you've experienced sudden vision changes or have been diagnosed with retinal vein occlusion, don't wait to get the specialized care you need.
Contact us today to schedule a comprehensive evaluation. Your vision is worth protecting, and we're here to help you do exactly that.